
Wellness's Safety Is What's Hurting People
The wellness industry counts the cost of being wrongly specific. It doesn't count the cost of being wrongly generic. The second is much bigger.
1. Why is Spotify more personalized than your fitness app?
Spotify can usually guess what I want to hear before I can.
Health apps still struggle to understand what to do with a woman in menopause who is losing bone and muscle, a 52-year-old man with hypertension on beta-blockers, or a person with ME/CFS or Long COVID whose body crashes 24 to 72 hours after ordinary activity.
That is not because music is more important than health. It is because music personalization is a preference problem. Health personalization is a care problem.
Spotify learns from dense, continuous, low-stakes feedback: what you search for, what you play, what you skip, what you save, what you exclude from your taste profile. Wellness learns from sparse, noisy, fragmented, high-stakes data — and usually without knowing the thing that matters most: who this body actually is, what else is going on in it, and what this person can safely do.
And yet the industry keeps saying personalized.
That is why everyone says it. And almost nobody means it.
2. What I mean by ‘no personalization in health’
I do not mean that wellness products do nothing adaptive.
They do. Apps personalize bedtime and exertion suggestions. They calculate readiness scores that move with your sleep. Some adapt training plans to hormonal phase. Some generate AI-driven workouts. Those are real forms of adaptation.
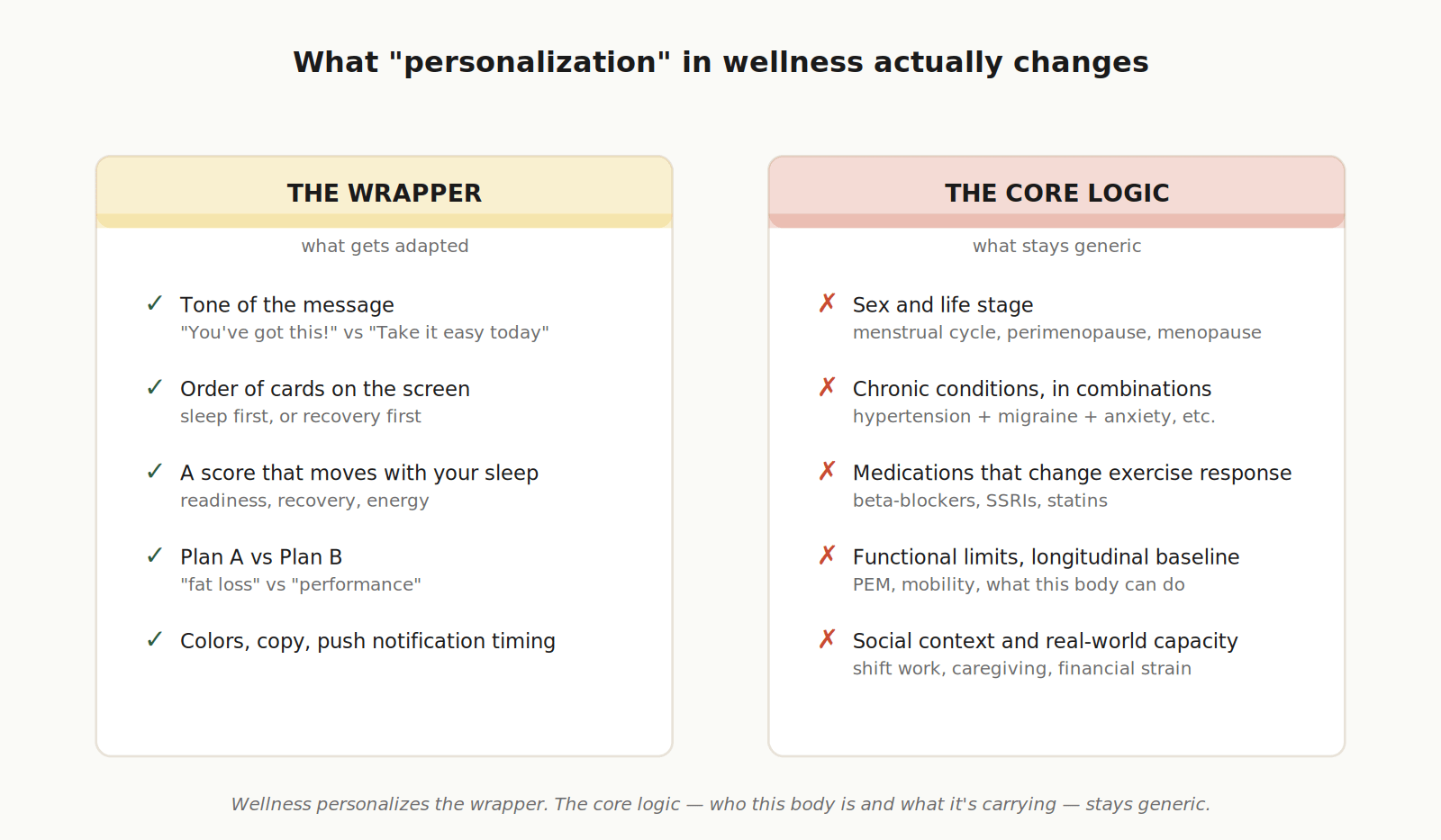
But they are usually not personalization in the health sense.
In health, personalization would mean that the core logic changes because of who the body is and what the body is carrying. It would have to change for:
sex and life stage,
chronic conditions and combinations of conditions,
medications that change exercise response,
longitudinal baseline and pattern over time,
functional limitations,
social context and real-world capacity.
If an app would still hand essentially the same recovery logic to a healthy 28-year-old, a woman in menopause, a man with hypertension on beta-blockers, a person with PEM, and someone with migraine + IBS + burnout, then it is not personalizing health. It is personalizing the wrapper.
A 2023 overview of personalized mHealth solutions found that these systems often rely on behavior-change theory, gamification, and motivational messaging, and “personalise the content rather than functionality.”1 That is the distinction the industry keeps blurring.
Tailoring content is not the same thing as personalizing care.
This is not unique to wellness. Even formal medicine is still mostly population-anchored. Eric Topol, writing in December 2024, made the point about ordinary lab tests: results are conveyed as “normal” or “abnormal” indexed to one-size-fits-all, population-based reference ranges — “for all the talk of ‘personalized medicine’ over the last two decades, this enriched interpretation of one’s lab test would be simple to implement.”2 If even clinical medicine, with a century’s head start, has not yet moved past the population average, the wellness layer downstream of it was never going to do that work on its own. The industry inherited a population-average frame and put a marketing layer on top.
That leaves a real question: if “personalization” today is mostly tailoring, what would actually solve this?
The fantasy answer is full individual personalization. Pure n=1. Every body modeled on itself, with no averages at all. That is not the answer either, and not for the reasons people usually give. We will come back to why. The short version: personalization in health is not a choice between the population average and the sample of one. The honest middle is phenotype-level — and that is the path this essay is arguing for.

3. Why almost every layer of the system rewards simplicity
This did not happen because founders are stupid or investors are cartoon villains.
It happened because complexity is expensive, and nearly every institution around health makes that expense someone else’s problem.
It started with the science.
Women are still meaningfully underrepresented in exercise and sport science. In one large audit across six major journals, female participants averaged only 34% of subjects, and only 6% of studies investigated exclusively women.3 The bias is not random. Female physiology — particularly across the menstrual cycle, perimenopause, and menopause — has historically been treated as more complex, more variable, and more expensive to study cleanly. So it got studied less. The NIH’s Office of Research on Women’s Health is candid about this: basic and preclinical biomedical research has “more often than not” focused on male animals and cells.4 Stacy Sims, the exercise physiologist who has spent more than a decade arguing this point, put it directly in May 2025: “Almost all the stuff you know with exercise and nutrition has been based on male data and generalized to women.”5 Much of what reaches consumers as “women’s wellness” is still adjusted male physiology, not a fully built female evidence base. Adding a cycle tab or a menopause filter does not solve the underlying gap. It personalizes the wrapper.
Medicine inherited the same instinct, in a different form.
Modern medicine has been organized around single diseases — diabetes, hypertension, depression, asthma — while real adult bodies increasingly carry several at once. The 2022 Nature Reviews Disease Primers synthesis of multimorbidity stated it as directly as a clinical journal will: most clinical practice guidelines and health-care training and delivery focus on single diseases, and that focus can produce care that is “sometimes inadequate and potentially harmful” for people with multiple conditions.6 It is much easier to build an app for “diabetes” or “sleep” or “stress” than for a person who is simultaneously living with hypertension, perimenopause, migraine, anxiety, and a parent in care. The first kind of product fits the science, the funding, the regulatory pathway, and the marketing language. The second kind of person is most of the user base.
That gap is so structural that funders had to build dedicated machinery just to study complexity at all.
The UK’s National Institute for Health and Care Research has an entire Multiple Long-Term Conditions research framework whose explicit aim is to change culture and practices to support this kind of work — reviewing funding processes, building multidisciplinary teams beyond single-disease specialisms, developing methods robust enough to handle complexity.7 That is a quiet institutional admission that the default research system was not built to produce person-level complexity well. It had to be retooled. The wellness layer downstream is even less equipped.
Startups and investors do not escape this either — and the irony is that the advice they receive is good advice, just not for this problem.
Early-stage companies are trained to survive by focusing. Y Combinator’s own essential startup advice tells founders that a small group of users who love them is better than a large group who kind of like them, and that early companies should focus on one or two key metrics.8 For most software, that is excellent advice. For real preventive health, it creates a structural trap. Because the human being who needs help rarely arrives as a clean wedge. She arrives as “menopause + insomnia + weight gain + anxiety.” He arrives as “hypertension + beta-blockers + deconditioning + bad sleep.” Another person arrives as “migraine + IBS + stress + fatigue.” The startup stack rewards one clean story, one ICP, one success metric, one fast roadmap. So founders simplify the human until the company becomes legible enough to fund, build, regulate, and market. That is not fraud. It is survival. It is also one of the reasons real personalization never quite shows up.
Then there is the regulation, which is the cleanest of all, because it is written into the rules.
The FDA distinguishes between low-risk “general wellness” products and products that move toward diagnosis, cure, mitigation, prevention, or treatment of disease. Software that is “maintaining or encouraging a healthy lifestyle” and unrelated to disease falls outside the device definition. Software that gets more disease-specific quickly enters a much harder regulatory world.9 So the market learned a very predictable lesson. It is much safer to say “optimize your sleep” or “boost recovery” or “train smarter” than to say “because you are on beta-blockers, the heart-rate logic this app normally uses may be wrong” or “because you have PEM, any fixed incremental increase in activity may backfire.”
The industry did not choose blandness by accident. It chose the side of the line that is easier to ship. By regulation, real personalization in health crosses into device territory. The wellness category is, by design, the un-individualized one. So when the industry says “personalized,” it is not lying — it is following the only definition of personalization that does not trigger a different regulatory regime. That is not a moral failure. It is a regulatory boundary doing exactly what it was built to do. But it also means the rest of us should stop pretending the word means more than the rules actually allow.
And on top of all of that, the hardest variable of all — the social and economic conditions in which a body is actually trying to live.
The WHO’s 2025 World Report on Social Determinants of Health Equity states it plainly: the conditions in which people are born, grow, live, work, and age — and the systems shaping access to power, money, and resources — can outweigh genetics, healthcare access, or personal choices in shaping outcomes.10 Does this person work shifts? Raise children alone? Live in chronic financial strain? Have time to recover, access to safe exercise, food that supports the plan? The body does not execute advice in a vacuum. A “personalized” plan that assumes stable sleep, discretionary time, and continuous adherence can be safe in every clinical sense and still be quietly impossible for the user it was supposedly built for.
None of this is anyone’s individual fault. The whole gravity field tilts toward simpler product, simpler claim, simpler user. Every layer independently pushes toward the same place.
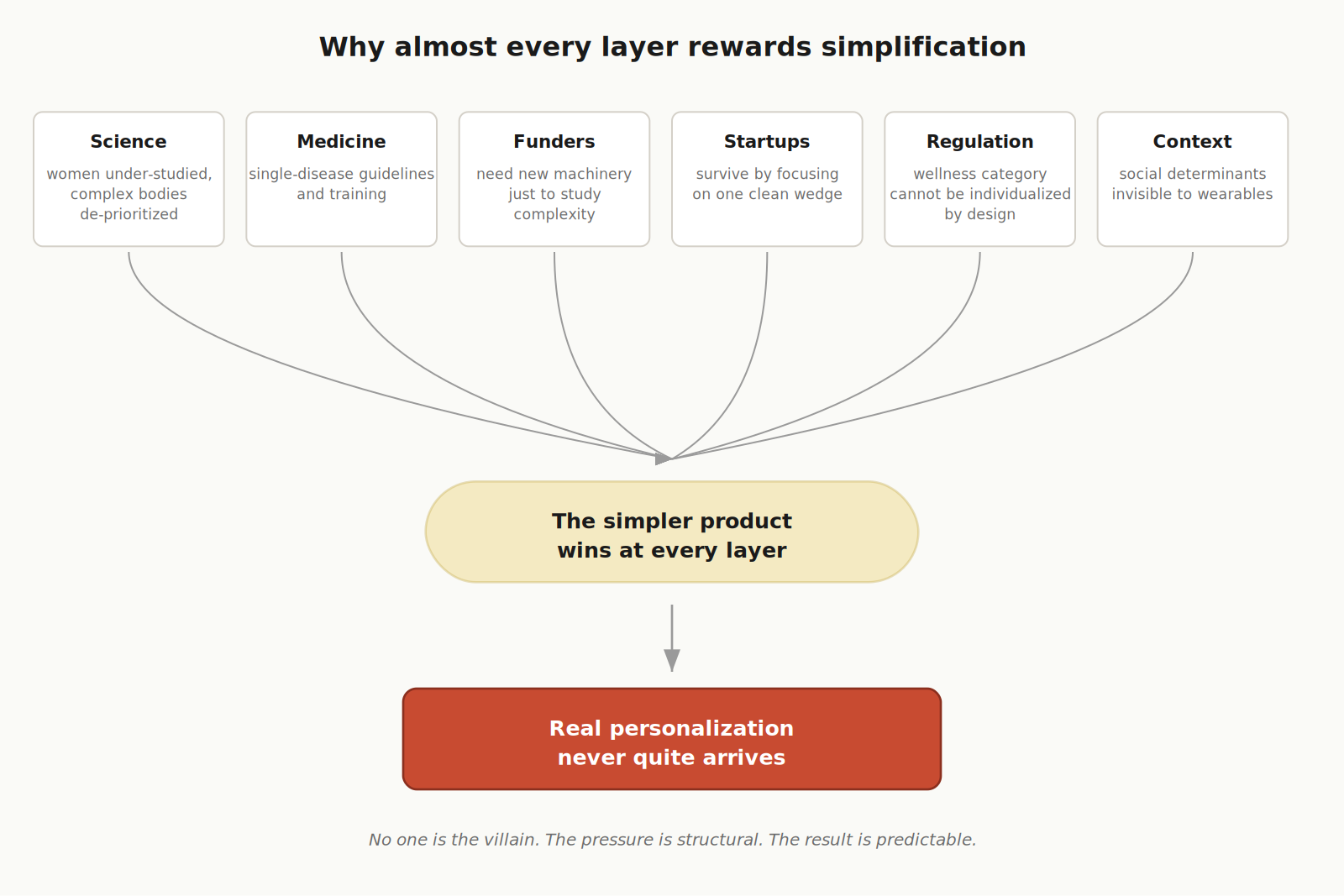
This is what I mean when I say no one is the villain. The pressure is structural. The result is predictable. And the cost — which we will turn to next — is not zero just because nobody is counting it.
4. The industry fears the wrong risk
There is a way the wellness industry talks about risk that, once you see it, becomes hard to unsee.
Health is terrified of commission error — saying something too specific and being wrong. Telling a beta-blocker user to chase a heart-rate zone that does not apply to them. Telling someone with ME/CFS to push through a crash. Telling a postpartum body to “get back in shape.” The fear is real, the liability is real, and the instinct to step back from disease territory is rational — especially under the FDA’s wellness lane, where staying broad and lifestyle-shaped is the price of remaining a wellness product at all.
But the industry is strangely comfortable with omission error — saying something so generic that it is wrong for millions of people, while still sounding safe.
Most of the industry has a sentence it does not quite say out loud, but acts on every day:
We treat bad personalization as dangerous.
We treat absent personalization as neutral.
It isn’t.
This is not a balanced risk calculation. It is an asymmetric one. The cost of being too specific is visible: a complaint, a regulator’s letter, a lawsuit, a feature pulled. The cost of being too generic is mostly invisible: it is the bone that was never preserved, the flare that was provoked, the wrong training zone that was chased for two years, the condition missed because the app kept talking to an “average” body, the right preventive behavior that was never started because the person received generic advice instead of relevant advice.
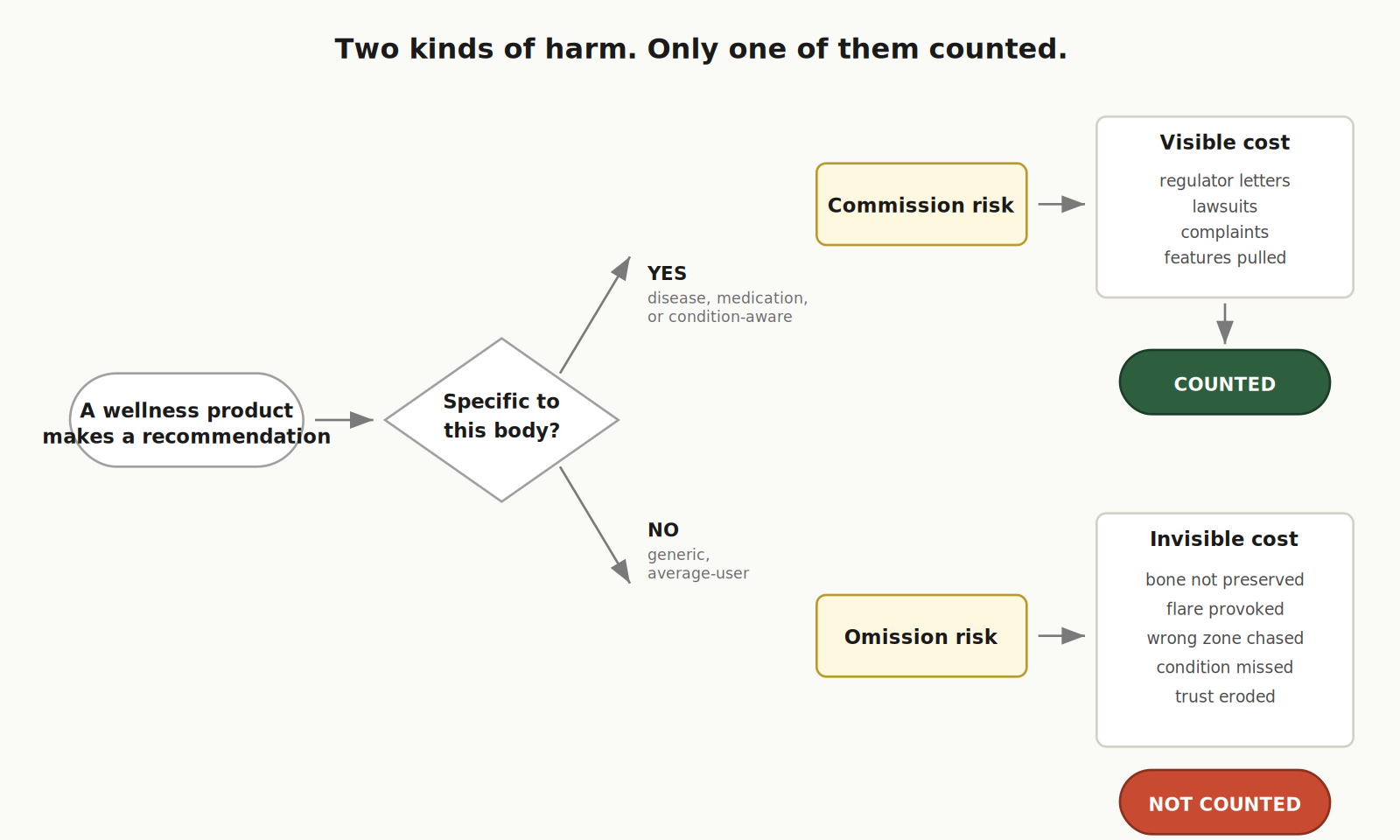
Nobody invoices the industry for these. Which is exactly why they keep happening.
What omission actually looks like
Three scenes make the asymmetry concrete.
Menopause. A woman in her early fifties opens her wellness app. It is supportive. It tells her to walk more, do yoga, breathe deeper, sleep better, be gentle with herself. She does all of it. Every day. For five years.
What the app never says, because it is not equipped to say it, is that the protocol her bones actually need is heavier than walking and harder than yoga. The Royal Osteoporosis Society is explicit: the best way to keep bones strong through and after menopause is both weight-bearing impact exercise and muscle-strengthening exercise.11 Neither is what her plan suggests.
She does not crash. She does not flare. She just quietly loses bone, year by year, doing exactly what the app told her was good for her. Twenty years later, what is gone is gone. Nobody marks it down as a product loss.
Hypertension and beta-blockers. A man in his early fifties starts a popular training app. He has hypertension. He is on beta-blockers. The app does not ask him about either. He picks a “smart” plan, puts on a chest strap, and starts training to heart-rate zones.
The trouble is invisible. Beta-blockers blunt heart rate by design. The American Heart Association is clear that target heart rate may need to be recalibrated with a clinician because these drugs affect everyone differently.12 Exercise is Medicine adds that on these medications, perceived effort is the safer guide than the number on the watch — and that if resting blood pressure climbs above certain thresholds, the right answer is not to train at all but to contact a doctor.13 None of that is in his app.
So he chases zones that do not apply to him. Sometimes he overshoots without realizing. Sometimes he undertrains because the number on his watch tells him he is fine. The app feels personalized. It is not. It is specifically wrong for him, and for several million people in the same situation. Almost nobody counts that damage.
PEM, Long COVID, ME/CFS. A woman in her thirties has had Long COVID for eighteen months. On a good day she can walk to the grocery store and back. On a bad day she cannot stand long enough to make coffee. Her wearable keeps congratulating her: streak achieved, ring closed, move goal exceeded. On the days she pushes for the green ring, she crashes for the next three.
The largest peer-reviewed Long COVID synthesis, published in Nature Reviews Microbiology in 2023, states it directly: “Some physicians, poorly educated in the aetiology and pathophysiology of the disorder, still advise patients to pursue harmful interventions such as graded exercise therapy and cognitive behavioural therapy, despite the injury that these interventions cause and the fact that they are explicitly not advised as treatments.”14 That is not fringe. That is the field’s own primary source. And the population it applies to is not small: KFF estimates that 17 million US adults — about 7 percent of all adults — currently report Long COVID.15
An entire class of mainstream wellness logic — step nudges, recovery scores that reward upward progression, “build capacity” framings — is not just unhelpful for this woman and the millions like her. It can actively make people worse, sometimes for years.
This is what omission looks like at scale. The system mistakes the wrong variable for the right one and, because it is still giving some recommendation, it treats itself as safe.

The economics of omission
The honest objection is: yes, but isn’t this all anecdotal? Where is the number?
There is no clean number, because no one counts omission as a category. But the size of the exposed population can be added up directly.
Hypertension affects 119.9 million US adults.16 Up to 3.3 million people in the US live with ME/CFS, at an annual economic burden the CDC estimates between $18 and $51 billion.17 About 59 million Americans provide unpaid adult care valued at roughly $1.01 trillion per year — a population whose plans of any kind are systematically misfitted to their available time and sleep.18 Approximately 3.6 million people enter postpartum physiology in the US every year, a life stage where generic “get back in shape” advice intersects with healing tissue, pelvic floor recovery, severe sleep loss, and elevated mood risk.19

Summed conservatively across just these four phenotypes — and they are far from the only ones — that is roughly 185 million annual person-phenotype exposures to wellness advice not designed for the person receiving it. The number is not unique people; overlap is heavy. It is the size of the population getting average-user advice in situations where average-user advice is the wrong tool.
We count the risk of saying the wrong specific thing.
We rarely count the risk of saying the wrong generic thing to 185 million people.
Trust is already paying the bill
There is one place where the cost of omission is showing up on a balance sheet: trust.
In Deloitte’s 2024 consumer health survey, the share of consumers who said they did not trust generative AI health information rose to 30 percent, up from 23 percent the year before — a seven-point drop in twelve months, in a category that depends on trust to function.20 You can argue about how much of that is AI-specific versus a broader signal about generic health content. But for a category that markets itself on being more personal, more responsive, and more aligned with the user than traditional medicine, a fall in trust at this speed should be read seriously.
People may not have the vocabulary for omission error. But they can feel when advice does not see them. And they are starting to act on it.
5. The average user is mostly fictional
When we talk about omission, it is tempting to picture an edge case — a small subset of unusual users who happen to fall outside the model. The population that does not fit the “healthy optimizer” frame is not the edge. It is the majority of the people the wellness industry is talking to.
Three-quarters of US adults have at least one chronic condition. Half have more than one. Even among 18-to-34-year-olds — the cohort wellness products most aggressively design for — six out of ten already have a chronic condition.21
And of the remaining quarter of US adults with no diagnosed chronic condition, the question becomes how many are actually metabolically healthy. The most recent NHANES-based analysis published in the Journal of the American College of Cardiology found that only 6.8% of US adults have optimal cardiometabolic health.22 Roughly one in fifteen.
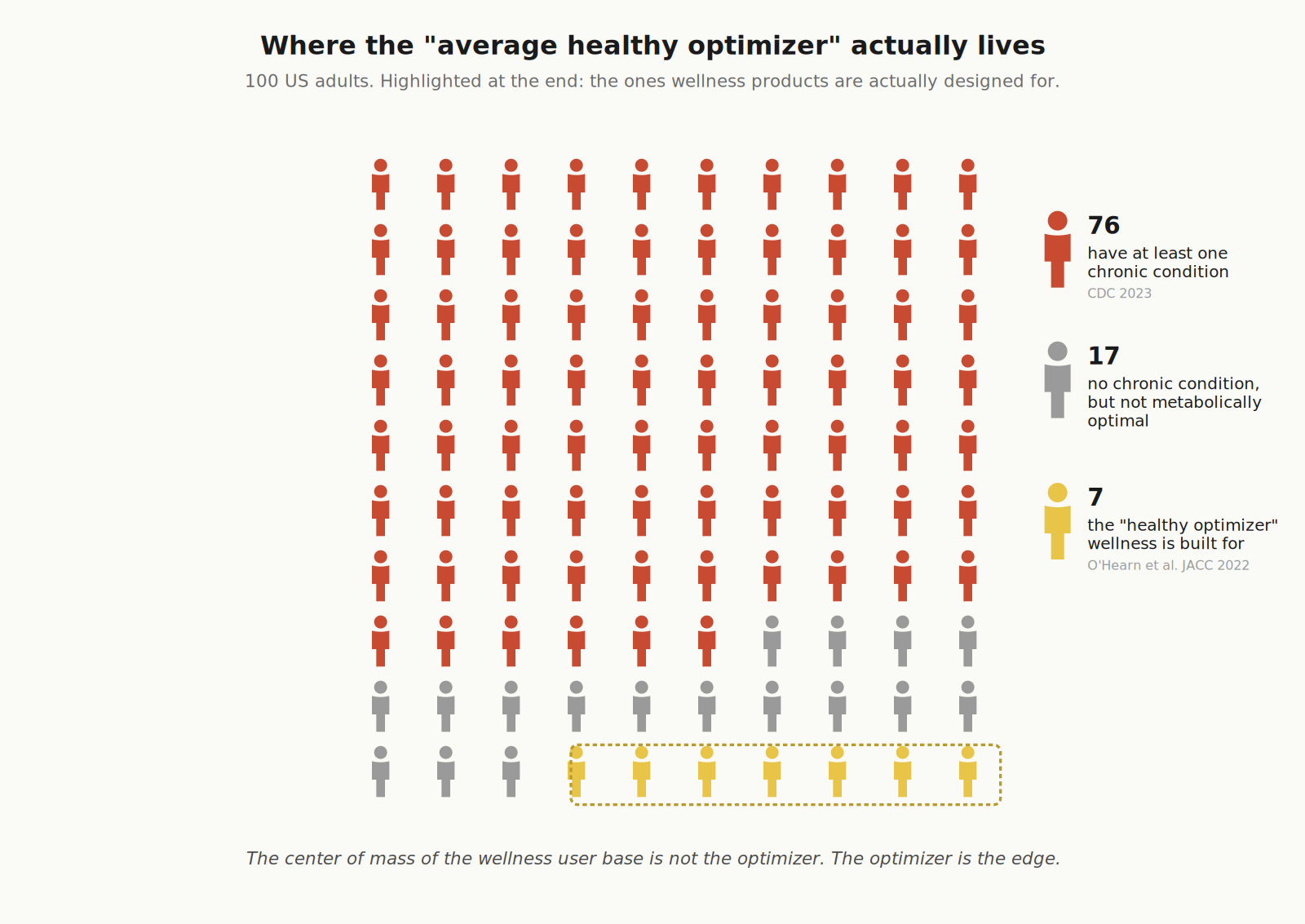
Wellness products design their core experience for the optimizer: someone with stable physiology, room to push, recoverable baselines, no medication interactions worth modeling. The data says that person is the edge of the user base, not its center. The actual center is someone managing one or more conditions, often invisibly, often without diagnosis, often without a vocabulary for what their body is doing.
The trend goes the wrong way, too. Between 2013 and 2023, the share of US adults aged 18-to-34 with multiple chronic conditions rose by roughly a quarter.21 The “healthy young adult” cohort is becoming a smaller share of the very age group wellness apps target most aggressively.
The average healthy optimizer is not the average. It is the rare exception. And the longer the industry designs as if it were the norm, the larger the omission burden becomes.
6. The bridge: phenotype-level personalization
If the wellness industry’s personalization is mostly tailoring, and “real personalization” sounds like science fiction, then the real product question is the one almost nobody asks honestly: what’s between them?
Why pure n=1 doesn’t work — and not for the reasons people usually give
The fantasy answer is full individual personalization. Every body modeled on itself. No averages. No cohorts. Just you, compared to your own setpoint.
That doesn’t work, and the problem isn’t compute or data. The problem is that pure n=1 leaves the user without orientation. You become your own scientist, running experiments on yourself, with a sample size of one. That isn’t care. It’s a research assignment most people didn’t sign up for.
When you feel worse than you did three months ago, “compared to your own baseline” tells you something has changed. It doesn’t tell you whether what’s happening to you is what happens to bodies like yours. Whether the people closest to your situation got better. What they did differently. What to try next. For most users, “be your own n=1” is not empowerment. It’s abandonment with a dashboard.
This is part of why we don’t think the future of health personalization is “n=1 for everyone.” That framing imports the same problem wellness has now, just flipped: the population-average frame strips away the individual; the pure-individual frame strips away the cohort. Both lose the same thing — the right reference class.
Three honest options
Once you accept that current wellness-personalization-as-tailoring is mostly marketing, and n=1 is mostly a fantasy in 2026, the real strategic question becomes a choice between three things.
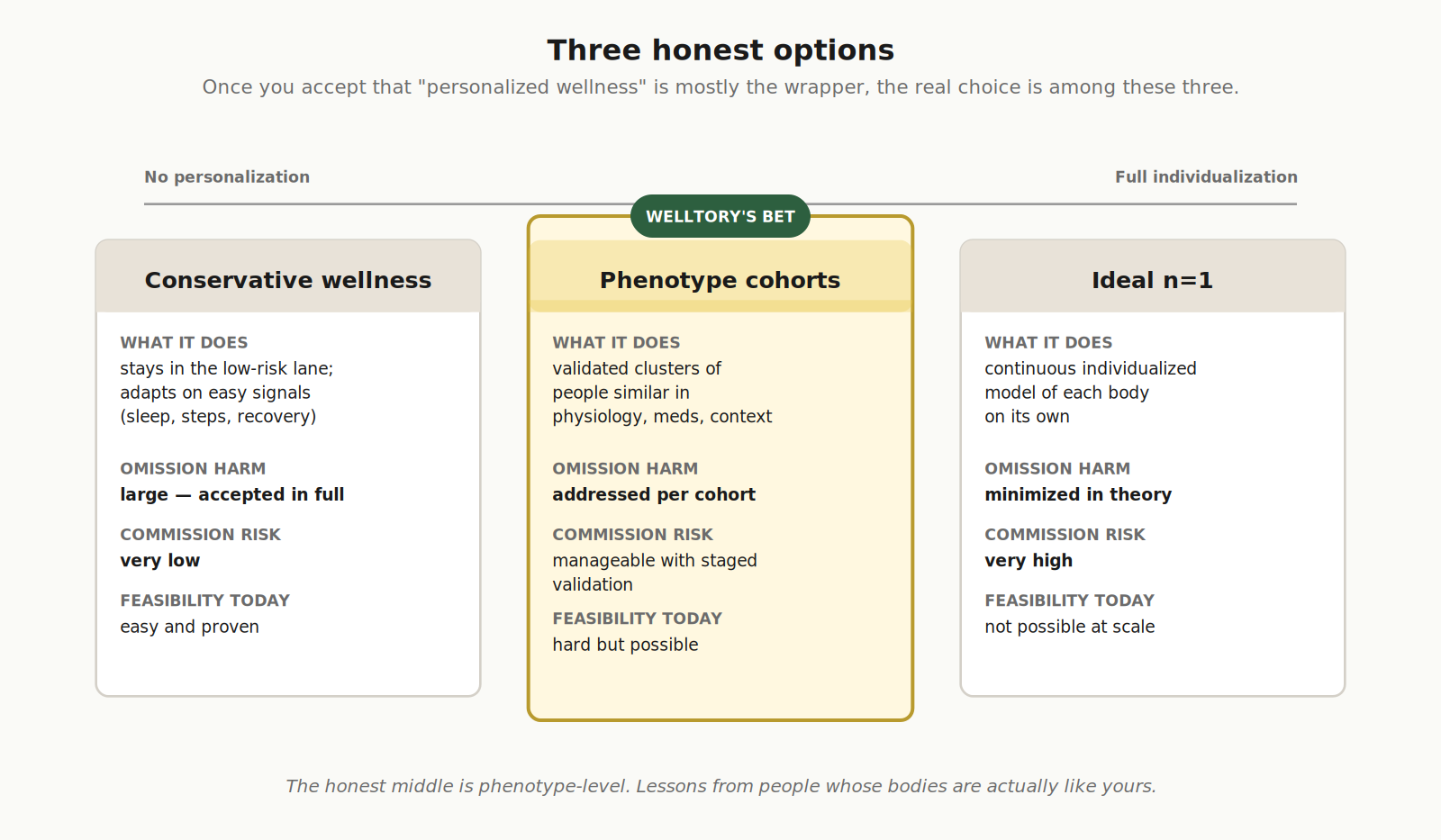
The honest middle is phenotype-level.
Why phenotype is the right reference class
A phenotype is not a marketing persona, and it is not a single diagnosis. It is a group of people who are genuinely similar in the ways that matter — symptoms, physiology, function, medication profile, life stage, social reality.
The reason this matters isn’t methodological elegance. It’s that humans learn by analogy to humans like themselves.
Every person who has ever joined a Long COVID Slack, a perimenopause subreddit, an ME/CFS Discord, an IBS support group, a fibromyalgia forum — what they’re looking for is not abstract averages, and not pure introspection. They’re looking for the right reference class. Other people whose bodies are doing something close enough that pattern recognition becomes possible. Recognition is the precondition for everything else: better questions, better experiments, better self-advocacy with clinicians, better predictions.
Phenotype-level personalization is the product version of that human instinct. Instead of comparing you to the population average (which you aren’t) or to yourself alone (which gives you no leverage), it compares you to the cluster of bodies actually doing what your body is doing. Advice can then be both specific and learned — without pretending to be omniscient.
That’s not a smaller idea than n=1. It’s a different idea. It scales. It can be validated. It can be improved one cluster at a time. And it gives the user the one thing pure self-measurement cannot give: other people.
The scale of what wellness ignores
This is where the abstract argument becomes a number.
If wellness products stay in the conservative lane — generic advice, untouched by phenotype — they leave the documented annual cost of every chronic phenotype they speak to fully in place. And those costs are not small.
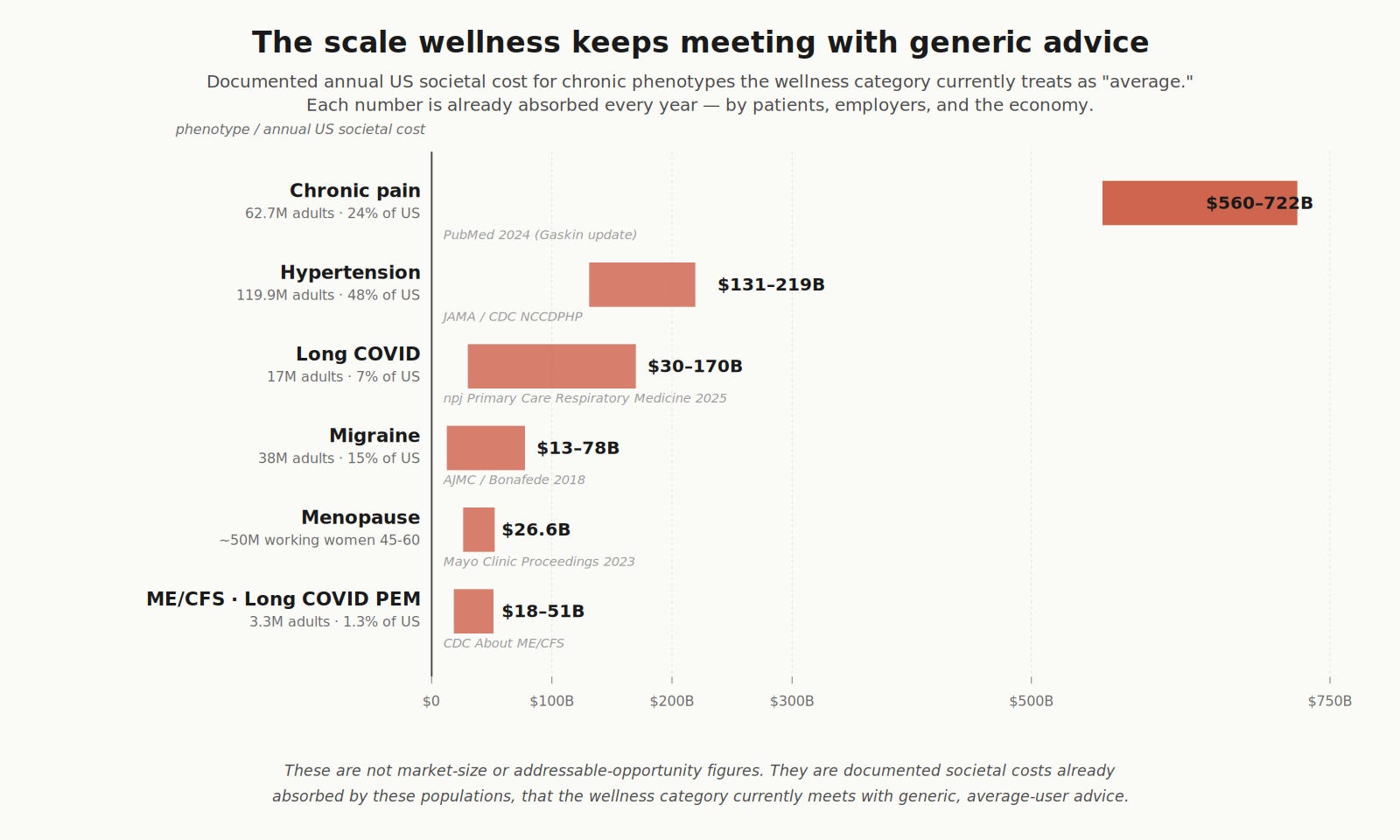
Hypertension: $131–219 billion in annual US societal cost.23 Chronic pain: $560–722 billion.24 Long COVID: $30–170 billion.25 Migraine: $13–78 billion.26 Menopause-related lost productivity and medical costs: $26.6 billion.27 ME/CFS: $18–51 billion.17 Each figure from CDC, peer-reviewed studies, or equivalent authority.
These are not market-size or addressable-opportunity numbers. They are documented annual societal costs — medical care, lost productivity, caregiver burden — already absorbed every year by patients, employers, and the broader economy, while wellness products continue to talk to these populations with logic built for a healthy 28-year-old optimizer.
The omission argument from earlier in this essay is not theoretical. The scale of what it ignores is, at minimum, this.

A worked example: ME/CFS
To make this concrete, here is the arithmetic for one phenotype where every input has a clean public estimate.
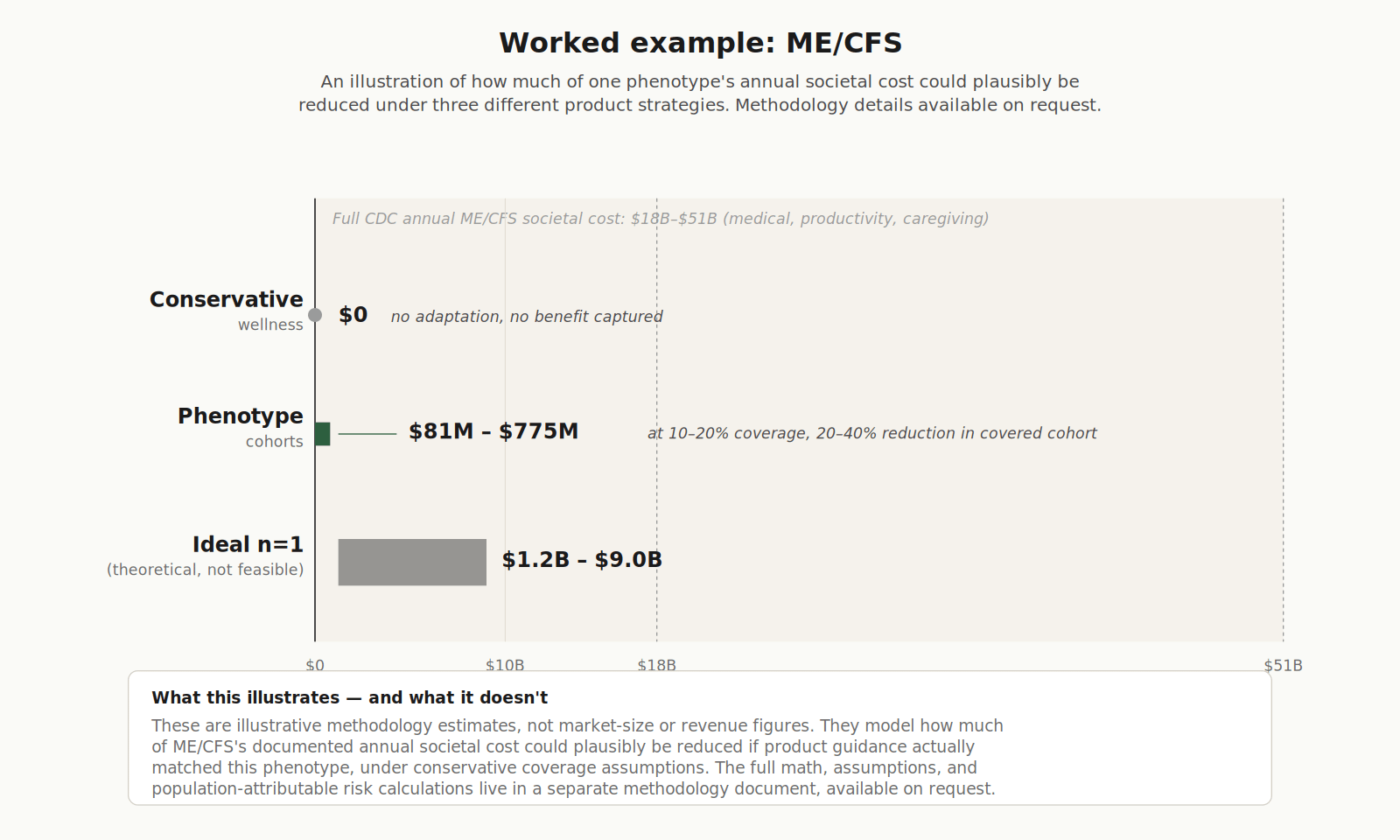
The annual societal cost of ME/CFS in the US is $18–51 billion (CDC). Under a “conservative wellness” strategy — generic advice, no phenotype-aware adaptation — essentially none of that burden is reduced. Under a phenotype-cohort strategy with deliberately conservative coverage assumptions, the order of magnitude lands in roughly $81 million to $775 million annually reducible. Under a theoretical “ideal n=1” strategy, $1.2–9 billion. But ideal n=1 is not feasible at scale in 2026, for reasons covered above.
I am not going to defend specific coverage numbers here — that work lives in a separate methodology document where the assumptions, the formulas, and the population-attributable risk math are visible to anyone who wants to argue with them.
The point is not the precision of any single number. The point is that the numbers exist at all — and that the wellness category’s current “be safe by staying generic” stance counts only the cost of being wrongly specific, while leaving the larger half of the equation uncounted.
That is why we are choosing the slow road — phenotype by phenotype, community by community, at the speed our resources allow. Not because it is fashionable, and not because it is easy. Because it is the only path between two failed ideas — generic wellness and impossible individual medicine — that actually adds up.
7. What we can no longer pretend at Welltory
We are not writing this from the outside.
We are part of this industry. And we are not writing this from finished work, either. We do not yet adapt our product well enough for PEM, for menopause, or for migraine + IBS — three of the phenotypes we already see most often in our own user base. We are not the worked example of what comes next. We are someone who has decided to stop being a worked example of what is wrong.
Two things we publicly stop doing.
We stop designing as if our average user is a healthy optimizer. The CDC says 76% of US adults have at least one chronic condition. Only 6.8% have optimal cardiometabolic health. That is not the edge of our user base. That is its center of mass. The healthy optimizer is the edge. From now on, that is how we treat the roadmap.
And we stop calling personalization what is not personalization. Adaptive messaging is not personalization. A score that changes with your sleep is not personalization. Plan A versus Plan B is not personalization. Real personalization in health changes the core logic of the product around the specific body in front of it — not the wrapper, not the copy, not the order of cards on a screen.
The rest is marketing.
8. So here’s what we’re actually doing
I could spend another section laying out principles for “responsible phenotype-aware personalization.” I’m not going to. The obstacles I described above are real, and I’ve spent months trying to find a way through them that doesn’t kill us under the complexity but actually lets us do something. This is what we landed on. It’s not a prescription for the industry. It’s just what we decided for ourselves.
We’re going to work phenotype by phenotype. One at a time. The mechanism is the same each time:
Launch a community cohort. Run the research jointly with the users in it. Build patient-led with medical advisors at the table. Study how their bodies actually work, what guidance actually helps, how the data we collect can support them inside the reality of their diagnosis — and we do all of that while staying inside what regulation actually allows so we don’t break anything we’d need later.
Then we move to the next phenotype and do it again.
We’ve already started. The first community is for people with post-exertional malaise — mostly women in their mid-forties to early sixties who have arrived at energy-limiting conditions through the same physiological pattern. We’ll see what comes out of it.
That’s the plan. Phenotype by phenotype. We don’t know yet if we’ll make it work at scale. We know the version of survival where we build the easier product and call it personalization isn’t a version we’re interested in. So we’re going to try this and see how far it takes us.
Phenotype by phenotype.
—
Jane Smorodnikova
Founder, Welltory
References
1. Iribarren SJ, Akande TO, Kamp KJ, Barry D, Kader YG, Suelzer E. “Designing personalised mHealth solutions: An overview.” International Journal of Medical Informatics (2023). https://www.sciencedirect.com/science/article/pii/S1532046423002216
2. Eric Topol, “Your Lab Tests.” Ground Truths Substack, December 14, 2024. https://erictopol.substack.com/p/your-lab-tests
3. Cowley ES, Olenick AA, McNulty KL, Ross EZ. “’Invisible Sportswomen’: The Sex Data Gap in Sport and Exercise Science Research.” Women in Sport and Physical Activity Journal 29(2):146–151 (2021).
4. NIH Office of Research on Women’s Health, “Sex as a Biological Variable.” Policy statement that basic and preclinical biomedical research has historically focused on male animals and cells, obscuring sex differences in health processes and outcomes. https://orwh.od.nih.gov/sex-gender/orwh-mission-area-sex-gender-in-research/sex-as-biological-variable
5. Stacy Sims, interview on The Dr. Hyman Show, “Women Are Not Small Men! Why Fitness Advice Is Failing Half the Population,” May 13, 2025.
6. Skou ST, Mair FS, Fortin M, Guthrie B, Nunes BP, Miranda JJ, Boyd CM, Pati S, Mtenga S, Smith SM. “Multimorbidity.” Nature Reviews Disease Primers 8, Article 48 (July 14, 2022). https://www.nature.com/articles/s41572-022-00376-4
7. National Institute for Health and Care Research, “Multiple long-term conditions (multimorbidity)” research framework and strategic priorities. https://www.nihr.ac.uk/explore-nihr/specialties/multiple-long-term-conditions.htm
8. Y Combinator, “YC’s Essential Startup Advice.” https://www.ycombinator.com/library/4D-yc-s-essential-startup-advice
9. U.S. Food and Drug Administration, “General Wellness: Policy for Low Risk Devices” — Guidance for Industry and FDA Staff. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/general-wellness-policy-low-risk-devices
10. World Health Organization, World Report on Social Determinants of Health Equity (2025). https://www.who.int/teams/social-determinants-of-health/equity-and-health/world-report-on-social-determinants-of-health-equity
11. Royal Osteoporosis Society, “Exercise for bone health.” Guidance that the best way to keep bones strong is to do both weight-bearing impact exercise and muscle-strengthening exercise. https://theros.org.uk/information-and-support/bone-health/exercise-for-bones/
12. American Heart Association, “How Do Beta Blocker Drugs Affect Exercise?” Notes that beta-blockers slow heart rate and that target heart rate may need to be recalibrated with a clinician. https://www.heart.org/en/health-topics/consumer-healthcare/medication-information/how-do-beta-blocker-drugs-affect-exercise
13. Exercise is Medicine / American College of Sports Medicine, “Exercising with High Blood Pressure.” Includes the do-not-exercise thresholds (systolic >200, diastolic >115) and guidance to use perceived effort over heart rate for those on beta-blockers.
14. Davis HE, McCorkell L, Vogel JM, Topol EJ. “Long COVID: major findings, mechanisms and recommendations.” Nature Reviews Microbiology 21, 133–146 (2023). https://www.nature.com/articles/s41579-022-00846-2
15. KFF, “As Recommendations for Isolation End, How Common is Long COVID?” Issue Brief, April 2024. Approximately 17 million US adults (~7%) currently report Long COVID. https://www.kff.org/coronavirus-covid-19/issue-brief/as-recommendations-for-isolation-end-how-common-is-long-covid/
16. Centers for Disease Control and Prevention, Million Hearts, “Estimated Hypertension Prevalence, Treatment, and Control Among U.S. Adults.” 119.9 million US adults (48.1%) have hypertension. https://millionhearts.hhs.gov/data-reports/hypertension-prevalence.html
17. Centers for Disease Control and Prevention, “About ME/CFS.” Up to 3.3 million US cases; annual economic burden estimated at $18–$51 billion. https://www.cdc.gov/me-cfs/about/index.html
18. AARP Public Policy Institute, “Valuing the Invaluable: 2023 Update — Strengthening Supports for Family Caregivers.” Approximately 59 million US adult caregivers providing unpaid care valued at $1.01 trillion annually. https://www.aarp.org/pri/topics/ltss/family-caregiving/valuing-the-invaluable.html
19. Centers for Disease Control and Prevention, National Center for Health Statistics, “Births: Provisional Data for 2024.” Approximately 3.6 million annual US births. https://www.cdc.gov/nchs/products/vsrr.htm
20. Deloitte Insights, “Build trust in health care gen AI” (Bill Fera, Jennifer A. Sullivan et al.), June 6, 2024. Share of consumers saying “I don’t trust the information” rose from 23% to 30% year-over-year. https://www.deloitte.com/us/en/insights/industry/health-care/consumer-trust-in-health-care-generative-ai.html
21. Watson KB, Carlson SA, Loustalot F, Town M, Eke PI, Thomas CW, Greenlund KJ. “Trends in Multiple Chronic Conditions Among US Adults, By Life Stage, Behavioral Risk Factor Surveillance System, 2013–2023.” Preventing Chronic Disease (CDC), April 2025. https://www.cdc.gov/pcd/issues/2025/24_0539.htm
22. O’Hearn M, Lauren BN, Wong JB, Kim DD, Mozaffarian D. “Trends and Disparities in Cardiometabolic Health Among U.S. Adults, 1999–2018.” Journal of the American College of Cardiology 80(2):138–151 (2022).
23. CDC NCCDPHP, “Health and Economic Benefits of High Blood Pressure Interventions.” Annual US costs associated with high blood pressure estimated at $219 billion (2019); the JAMA AHA series (Kirkland et al.) estimates $131 billion in annual incremental healthcare expenditures across 2003–2014. https://restoredcdc.org/www.cdc.gov/nccdphp/priorities/high-blood-pressure.html
24. Wieder et al., “Economic Costs of Chronic Pain — United States, 2021.” Medical Care (2025). Estimates $722.8 billion annual US cost, including $530.6B medical care and $192.2B lost productivity. https://pubmed.ncbi.nlm.nih.gov/40730349/
25. npj Primary Care Respiratory Medicine, “Economic burden of long COVID: macroeconomic, cost-of-illness and microeconomic impacts” (2025). Estimates annual US lost earnings of approximately $170 billion. Companion estimate from Bartsch et al., Journal of Infectious Diseases (2025): $2B–$31B annually depending on symptom duration. https://www.nature.com/articles/s41533-025-00460-8
26. Bonafede M et al., “Direct and Indirect Healthcare Resource Utilization and Costs Among Migraine Patients in the United States.” Headache: The Journal of Head and Face Pain (2018). Reports total annual US migraine cost of approximately $36 billion. Broader estimates from neurological disease reports reach $78 billion. https://www.ajmc.com/view/study-summary-costs-associated-with-migraine-in-the-united-states
27. Faubion SS et al., “Impact of Menopause Symptoms on Women in the Workplace.” Mayo Clinic Proceedings (2023). Reports $1.8 billion in annual lost work time and $24.8 billion in annual direct medical costs in the US, totaling $26.6 billion. https://newsnetwork.mayoclinic.org/discussion/mayo-clinic-study-puts-price-tag-on-cost-of-menopause-symptoms-for-women-in-the-workplace/